
Lee A. Fleisher, MD
- Robert D. Dripps Professor and Chair
- of Anesthesiology and Critical Care
- Professor of Medicine
- University of Pennsylvania School of Medicine
- Philadelphia, Pennsylvania
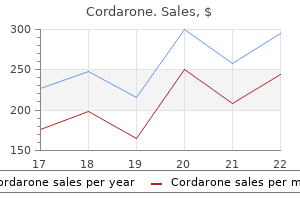
Autonomic nervous system state: the effect of general anaesthesia and bilateral tonsillectomy after unilateral infiltration of lidocaine treatment 2 prostate cancer 100mg cordarone sale. Effect of fentanyl on heart rate variability during spontaneous and paced breathing in healthy volunteers medicine video cheap cordarone 200 mg free shipping. The influence of xewnon on regulation of the autonomic nervous system in patents at high risk of periperative cardiac complications symptoms zoloft dosage too high 100 mg cordarone free shipping. Cardiac sympathovagal balance and peripheral sympathetic vasoconstriction: epidural versus general anesthesia treatment programs cordarone 100mg for sale. Heart rate variability: a diagnostic and prognostic tool in anesthesia and intensive care. Pulsatile signaling and cardiovascular aging: functions and regulation of natriuretic peptide signaling. Peripheral mechanisms of thermoregulatory control of skin blood flow in aged humans. Ritchie, Assistant Inspector General for Audit Services, Office of Inspector General, U. Present: Senators Johnson, Daines, McCaskill, Carper, Heitkamp, Hassan, Harris, and Jones. The first chart1 just shows who pays for health care as a percentage of total health care spending. You can see the trend since 1940 where patients were paying more than 80 cents out of every dollar. So what we have seen is a huge shift from patients being connected to the payment of the product to that disconnect. And when patients do not pay for products, they do not even know what they cost, and so there is not that discipline of a free market really disciplining the cost increase in health care. And from my standpoint, that is the root cause of our broken health care financing system, which is why health care costs have really risen dramatically. When you remove the discipline of the free market system in terms of ensuring the highest possible quality, lowest possible cost, best possible level of customer service, you see costs rise dramatically. Now, we also can do far more-and this is a good thing-in terms of our medical system. But I have to believe the fact that consumers really do not care-they do not know what things cost, and they really do not care, other than their insurance. They really care about how much they pay for insurance, but the individual health care items, they really do not care. Now, what I would say, truthfully, if Americans are spending their own money and in freedom were deciding to spend 17 percent of their disposable income on improving their health, I would not have a problem with that. But because they are not spending their own money directly for this, I think this is a real distortion of the marketplace. The next chart3 is total Medicaid spending, which is really the subject of the hearing today in terms of why we have to be very careful with taxpayer dollars. Medicaid was not even mentioned by Lyndon Johnson when he unveiled Medicare, but you can see the dramatic increase in Medicaid spending. Just in the last 10 years, it has more than doubled, from right around $200 billion to $430 billion. Now, in our report we show that total taxpayer spending on Medicaid in 2017 was $554 billion. Which, when you take a look at what the Federal Medicaid percentages should be, somewhere between 58 and 60 percent, we are only seeing $124 billion spent by the States versus $430 billion spent by the Federal Government. What happens-and it drives me nuts being an accountant-numbers come from different sources, and it is very difficult to reconcile. That is something, as I am preparing for the hearing, that just jumped off the page for me. Why is that such a disconnect from, let us say, the 60 percent Federal match to this thing shows almost 78 percent? In 2017 it was $37 billion, the largest percentage of any agency, any program in the Federal Government in terms of improper payments. Coming into this role, I always thought the term ``improper payment' was a little odd because it covered both underpayment and overpayment. So this is payments that should not be made, whether they are to ineligible recipients, what percent of that is fraud. So we will be talking about a letter we got from Administrator Verma yesterday announcing increased action on this, audits, those types of things.
Diseases
- B-cell lymphomas
- Gougerot Sjogren syndrome
- Hemolytic anemia lethal genital anomalies
- Developmental delay epilepsy neonatal diabetes (DEND syndrome)
- Acromegaloid facial appearance syndrome
- Placental abruption
- Essential hypertension
- Paraparesis amyotrophy of hands and feet
- Fetal antihypertensive drugs syndrome
- Systemic necrotizing angeitis
The strongest predictors of persisting distress included being female medicine hat news cheap cordarone 100 mg with amex, having less than a high school education symptoms vitamin b12 deficiency buy discount cordarone 100mg line, being middle-aged and having more than two diabetes-associated biomedical complications [40] medicine keri hilson lyrics cordarone 100 mg discount. An early analysis of 42 studies indicated that the risk of depression was doubled in people with diabetes symptoms sleep apnea order cordarone 250mg visa, as compared to people without diabetes, and this occurred regardless of type of diabetes (Figure 49. Clinically significant mood disorders in adults the process of psychologic adaptation to the diagnosis of diabetes in adulthood remains incompletely understood, largely because few longitudinal studies have been conducted with adults [29]. Rates of clinically significant distress were higher in both treatment groups (25%) compared with rates of depression measured by self-report in the general population (14. The data are from a meta-analysis of 42 studies; figures for subjects with diabetes are the aggregate of both controlled and non-controlled studies. Psychologic Factors and Diabetes Chapter 49 Variations in prevalence rates are common across individual studies, and appear to be related to the method used to ascertain depression. Those studies using self-report symptom scales yielded prevalence rates that were nearly three times higher than rates obtained using formal structured interviews with clinically established diagnostic criteria (31% vs 11%) [32]. Discrepancies amongst studies have also been found to be caused by differences in subject characteristics, particularly age and medical history [45,46]. The highest rates of current psychiatric distress tend to be found in hospitalized patients [47] or in older adults with multiple medical co-morbidities [48,49]. Frequently [50,51], but not invariably [45,52], adults with diabetes and more emotional problems also have poorer metabolic control. A review of more than 30 studies indicates that although depression is associated with higher HbA1c values, the magnitude of this effect is extremely small, with the exact value being a function of how depression is ascertained. In studies using symptom self-reports, less than 3% of the variance in HbA1c was explained by depression; when standardized diagnostic interviews are used, approximately 8% of the variance in HbA1c was accounted for by depression [53]. Studies of children with diabetes have indicated that the best predictor of future psychopathology is past psychopathology [16], and the same principle applies to adults. Repeated episodes of depression were common in the initially depressed group, with subjects having an average of 4. Recurrence of depression was apparently unrelated to duration of disease, type of diabetes or development of diabetes-associated complications, but it was associated with a family history of psychiatric disorder. A subsequent study found that the severity of recurrent depressive episodes was related to the presence of neuropathy, but no other biomedical complication, at study entry and it has been suggested that the discomfort associated with this complication may serve as a stressor capable of provoking an episode of depression in vulnerable individuals [54]. The generally weak relationship between diabetes-related variables and reoccurrence of a mood disorder suggests that depression is not merely a psychologic reaction to the development of diabetes or its complications, but may be influenced significantly by underlying genetic or constitutional factors [25,55,56]. Although the exact pathologic mechanisms have not yet been established, it is certainly plausible that depression could greatly increase the likelihood of developing diabetes, in so far as depressive symptomatology is associated with a variety of behavioral. The diagnosis and treatment of depression and other psychiatric disorders in patients with diabetes is described in detail in Chapter 55. In the same way that the child recently diagnosed with diabetes manifests an anxious or depressed mood as part of an adjustment disorder, older patients might be expected to show psychologic distress soon after a complication appears. This conjecture has not been tested empirically: it is not known how adults with diabetes react psychologically shortly after a complication appears, although as a group, adults with complications usually [61], but not invariably [62], have greater levels of psychologic distress. Three types of diabetic complications are known to increase the risk of psychopathology: macrovascular disorders, chronic foot ulceration and sight-threatening proliferative retinopathy. Adults with diabetes and macrovascular disease often have elevated rates of depression [52] and poorer quality of life [55], although this is not always the case [46,63]. Similarly, patients with chronic unilateral foot ulceration secondary to diabetic neuropathy have higher rates of depression and report greater dissatisfaction with their lives than age-matched adults with diabetes but no history of foot ulceration [64]. Results from a prospective cohort study noted that 24% of adults with diabetes presenting with their first diabetic foot ulcer had clinically significant major depression, and this was associated with a threefold risk of death during an 18-month follow-up period [65]. Other studies have also demonstrated marked increases in depressive symptomatology and peripheral neuropathy, and have attributed this psychologic distress to the physical distress associated with reduced feeling in the feet and unsteadiness, as well as its unpredictability [66,67]. Increased psychiatric symptomatology is also seen in patients with proliferative diabetic retinopathy, compared with those without retinopathy [68]. In a meta-analysis that included 13 811 Part 9 Other Complications of Diabetes of visual problems affect mental health.
Discount 200mg cordarone with mastercard. First Month of Pregnancy Symptoms -- Early Pregnancy Symptoms.
A vagal neuropathy can cause antral hypomotility and/or pylorospasm treatment sinus infection cheap 200 mg cordarone visa, which may delay gastric emptying [23] symptoms questionnaire order cordarone 200mg with amex. The pathophysiology of rapid gastric emptying in diabetes is less well understood medicine you cannot take with grapefruit cordarone 250mg online. Conceivably medicine 44-527 buy cordarone 250 mg fast delivery, impaired gastric accommodation resulting from a vagal neuropathy [24] may increase gastric pressure and thereby accelerate gastric emptying of liquids. The relationship between vagal neuropathy and impaired post-prandial accommodation is unclear because accommodation may be preserved even in people with diabetes and vagal neuropathy [25], perhaps reflecting non-vagal adaptive mechanisms involving enteric neurons [26]. Some patients with diabetes and gastroparesis also have small intestinal dysmotility, more frequently characterized by reduced than by increased motility [27]. Diabetic diarrhea It is useful to categorize the pathophysiology of diabetic diarrhea into conditions that are associated with malabsorption and those that are not (Figure 46. Involvement of sympathetic fibers, which normally inhibit motility and facilitate absorption via 2adrenergic receptors, can result in accelerated small intestinal transit and cause diarrhea [38]. Patients with rapid ileal transit may have bile acid malabsorption [39,40] and deconjugated bile acids induce colonic secretion. Features suggestive of malabsorption such as anemia, macrocytosis or steatorrhea should prompt consideration of bacterial overgrowth, small bowel mucosal disease or pancreatic insufficiency. Small intestinal dysmotility predisposes to bacterial overgrowth, which can cause bile salt deconjugation, fat malabsorption and diarrhea. Chronic pancreatic insufficiency may result from pancreatic atrophy, disruption of cholinergic enteropancreatic reflexes, or elevated serum hormonal levels of glucagon, somatostatin and pancreatic polypeptide, which reduce pancreatic enzyme secretion [42]. Nevertheless, the association between chronic pancreatic insufficiency and diabetes is uncommon. These effects may be explained by hyperglycemia-induced suppression of antral motility and migrating motor activity, the so-called intestinal "housekeeper" [3234]. Acute modulation of blood glucose within the physiologic postprandial range (48 mmol/L) can also delay gastric emptying, to a lesser degree [31]. Cross-sectional studies suggest that higher glycated hemoglobin concentrations are associated with a higher prevalence of gastrointestinal symptoms and slower gastric emptying among people with diabetes in the community [6,35]. While strict glycemic control improves neural, renal and retinal functions in diabetes, the impact on gastric emptying is unclear [36]. In addition to hyper- 764 Gastrointestinal Manifestations of Diabetes Chapter 46 only 10% of pancreatic function is sufficient for normal digestion. Because of the high prevalence of coronary atherosclerosis in diabetes, testing for coronary artery disease should be considered when necessary in patients with chest pain. Fecal incontinence Loose stools and anorectal dysfunctions contribute to fecal incontinence in diabetic diarrhea. Compared to continent people with diabetes and healthy controls, patients with diabetes and fecal incontinence have a higher threshold for rectal perception of balloon distention, a marker of reduced sensation [43,44]. A sympathetic neuropathy may impair internal anal sphincter function and anal resting pressures while a pudendal neuropathy may result in reduced anal squeeze pressure. Dyspepsia and gastroparesis Although gastroparesis refers to a syndrome characterized by symptoms of nausea, vomiting, early satiation after meals and impaired nutrition and objective evidence of markedly delayed gastric emptying, gastric retention may be asymptomatic [50], perhaps because of the afferent dysfunction associated with vagal denervation [51]. Nausea and vomiting may be associated with impaired glycemic control and often cause hypoglycemia, perhaps because delivery of food into the small bowel for absorption is not sufficient to match the effects of exogenous insulin. Consistent with the concept of a paralyzed stomach, the term gastroparesis should be restricted to patients with markedly delayed gastric emptying. When the delay in gastric emptying is not severe, the term diabetic dyspepsia is perhaps more appropriate. Dypepsia is characterized by one or more, generally postprandial, upper gastrointestinal symptoms, including bloating, post-prandial fullness and upper abdominal pain. Typically, vomiting is not severe but significant weight loss secondary to reduced caloric intake is not unusual. In addition to delayed gastric emptying, impaired gastric accommodation and abnormal, either increased or decreased, gastric sensation may also contribute to symptoms in diabetes [52,53].
Prunus serotina (Wild Cherry). Cordarone.
- How does Wild Cherry work?
- Dosing considerations for Wild Cherry.
- Are there any interactions with medications?
- Cough, colds, bronchitis, diarrhea, and other conditions.
- What is Wild Cherry?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96856
References
- Du MQ, Diss TC, Dogan A, et al. Clone-specific PCR reveals wide dissemination of gastric MALT lymphoma to the gastric mucosa. J Pathol 2000;192:488.
- Goodman JL. Possible transmission of herpes simplex virus by organ transplantation. Transplantation. 1989;47:609-613.
- Boudreau S, Hines HC, Hood AF: Dermal abscesses with Staphylococcus aureus, cytomegalovirus and acid-fast bacilli in a patient with acquired immunodeficiency syndrome (AIDS). J Cutan Pathol 15:53-57, 1988.
- Maron BJ, Applefeld JM, Krovetz LJ. Racial frequencies in congenital heart disease. Circulation. 1973; 47:359-61.














