Peter J McDonnell, M.D.
- Director of The Wilmer Eye Institute
- Professor of Ophthalmology

https://www.hopkinsmedicine.org/profiles/results/directory/profile/0003333/peter-mcdonnell
Each of these contributes to changes in the optical length and resonant frequencies of the laser cavity cholesterol medication powder discount prazosin 5mg with amex. These changes are especially significant in miniature lasers where the active volume of the gain medium constitutes much of the resonator cholesterol level chart in urdu safe prazosin 5mg. Internal stress leads to stress birefringence and cholesterol no longer bad effective 5 mg prazosin, eventually cholesterol foods high list order 5mg prazosin, stress-induced fracture. Other issues that must be considered in high-power lasers are nonlinear optical effects and optical damage. The electrical field within the optical beam of a high-power laser can be large enough to damage optical components. This is particularly important in high-peak-intensity pulsed lasers such as passively Q-switched microchip lasers. As a result, miniature lasers are usually designed to operate in the fundamental transverse mode. Most of the results and formulas presented in this section are derived for fundamental-mode operation and may require some modification for lasers operating in multiple transverse modes. The transverse modes of a laser are determined by the cavity design and the pump-energy deposition profile. The cavities for many miniature solidstate lasers are small versions of larger devices, designed according to the same principles (Hall and Jackson, 1989). However, the use of longitudinal pumping allows additional possibilities for obtaining stable cavity modes. The planar uniformity of such a cavity is broken by the pump beam, which deposits heat as it pumps the crystal. The heat diffuses away from the pump beam, generally resulting in a radially symmetric temperature distribution. In addition, when the cavity mirrors are deposited on the gain medium, there is some thermally induced curvature of the mirrors as the warmer sections of the gain medium expand or contract. In materials with a positive thermal expansion coefficient e this effect also contributes to the stabilization of the transverse mode. Another effect is strain-induced variation of the refractive index caused by nonuniform heating and expansion of the gain medium. This effect tends to be less important than the others in determining the transverse mode characteristics of the cavity, although it can cause local birefringence. For the case of nonuniform heating, the thermal expansion of the warmer sections of the material will be constrained by the cooler regions, and C may be a function of the thermal gradients. If the cavity length is short compared to the confocal parameter, as in the case of microchip lasers, the total change in optical length as a function of transverse cavity position can be modeled as a simple lens between the two flat mirrors or as an axially uniform waveguide with a radially varying index. For a monolithic, longitudinally pumped, short cavity with radial heat flow, the radius of the oscillating mode rm is given by (Zayhowski, 1991a) 2 (r02 + rp)lkc r = o, Pan nl,T 2 m 1/ 2 (1. Once nl,T and r0 are determined, this equation does an excellent job of describing the pump-power dependence of the oscillating-mode radius for many microchip lasers. The maximum angle max that can be tolerated between the mirrors (for symmetric fundamental-mode operation) is given by (Zayhowski, 1991a) max = 1. It is usually insignificant compared to thermal guiding but can be important in low-duty-cycle lasers where thermal effects are minimized. Near threshold there is little saturation of the population inversion, the round-trip amplification of the mode is highest near the center of the mode, and gain guiding will tend to reduce the mode cross section. Well above threshold the population inversion at the center of the mode is saturated and residual gain in the wings (if there is any) can lead to a slight increase in the mode radius (Kemp et al. Laser modes that are spectrally detuned from the center of the gain profile will see a refractive index that is a function of their detuning. Modes that fall on the long-wavelength side of the gain profile will see an increased refractive index; modes on the short-wavelength side will see a decreased refractive index. If we assume a Lorenzian gain profile, the change in refractive index seen by a mode as it moves away from the gain peak is n(r, z,) = 0 (- 0) g(r, z,), 2 (1. Hence, n(r,z,) depends on the mode profile and must be calculated self-consistently. In either case, the deformation of the optical path near the center of the mode, due to gain-related index guiding, can usually be modeled as a spherical (positive or negative) intracavity lens. As a result of gain-related index guiding, each of the longitudinal modes of a laser has a slightly different spatial profile, a different amount of overlap with the pump, and a different far-field divergence.
It is then conducted by the bundle of His down the septum high cholesterol definition wikipedia effective 2.5mg prazosin, and out into the ventricular walls by the Purkinje fibers does cholesterol medication remove plaque arteries purchase prazosin 2.5 mg with amex, causing 494 Appendix Figure A usda cholesterol in eggs generic prazosin 2.5 mg free shipping. On the left is a heart showing the sinoatrial (pacemaker) node cholesterol levels mmol/l conversion discount prazosin 5 mg mastercard, the atrioventricular node, the bundle of His, and the Purkinje fibers, comprising the right, left anterior, and left posterior bundle branches. Numbers on the heart show typical contraction times after the discharge of the sinoatrial node, in milliseconds. Notice that the impulse is delayed at the atrioventricular node before being conducted down the ventricular septum by the bundle of His. The delay is necessary to allow the ventricles to fill with blood during atrial contraction before the ventricles themselves contract. In interpreting the positions of the conducting fibers in this diagram, it should be remembered that the fibers run in the three-dimensional tissue of the heart and therefore can only be shown approximately in a two-dimensional cross-section as shown here. This is because the spatial pattern of ventricular repolarization is different than that of ventricular depolarization. The Physiology of Excitable Cells, 2nd edn (Cambridge: Cambridge University Press, 1978). James Adams and his tradition of generating practical, up-to-date and evidence-based guidelines that provide bedside clinicians with a ready reference for patient care. The editors, section editors, and various authors have worked hard to preserve relevant material from the guidelines and add new relevant information. Community neonatology colleagues, nurse practitioners, dietitians, and fellows are all members of author teams now. It ensures consistency of care among the large number of clinicians in our Newborn Center and at multiple locations in the Houston area. It has been, and will remain one of the most valuable resources and a distinguishing asset of the Neonatology Section. As the Service Chief and Section Head of Neonatology, it has been my honor to support the team of editors and authors who have worked hard to bring us this distillation of evidence, experience, and clinical wisdom. This body of work is reflective of general principles, concepts, and treatment recommendations that are agreed upon by the authors, editors, and section members. When appropriate, national guidelines are cited to help with the decision-making process. Also, regional traits unique to the southeast Texas or Houston are considered when appropriate. The guidelines are reviewed and revised annually (or more frequently as needed) as new evidence and recommendations for clinical care become available. Our guidelines cite the quality of evidence and the strength of our recommendations whenever possible. Our chapter authors and section editors have worked hard to create the content you see within and will monitor their areas of clinical interest for emerging evidence that may be of value to the bedside clinician caring for a sick neonate. Each new admission and all significant new developments must be discussed with the fellow on call and with the attending neonatologist on rounds. All users of this material should be aware of the possibility of changes to this handbook and should use the most recently published guidelines. Infectious Disease section was written with the advice of the Pediatric Infectious Disease Section, in particular, Drs. If servo- control mode of incubator is used, indicate servo skin temperature set point (usually set at 36. If only radiant warmer is available use plastic wrap blanket to reduce evaporative water loss for babies who weigh 1250 grams or less. Oximeter - oxygen saturation target 90-95% for premature infants and term babies with acute respiratory distress (alarm limits 88-96%). Vital signs and blood pressure by unit routines unless increased frequency is indicated.

Hypoglycemia Risk Preventing hypoglycemia is the most critical and challenging safety issue for any driver with diabetes mellitus definition of cholesterol in nutrition generic 2.5 mg prazosin with amex. Rescue Glucose In some cases cholesterol levels ratio calculator discount 5 mg prazosin with mastercard, hypoglycemia can be self-treated by the ingestion of at least 20 grams of glucose tablets or carbohydrates cholesterol medication mechanism of action buy prazosin 2.5mg overnight delivery. Consuming "rescue" glucose or carbohydrates may avert a hypoglycemic reaction for Page 178 of 260 less than a 2-hour period lowering cholesterol tlc diet generic 2.5mg prazosin with amex. The driver with a diabetes exemption must carry a source of rapidly absorbable glucose while driving. In the last 5 years, has had recurring (two or more) disqualifying severe hypoglycemic reactions (as described above). Blood Glucose Poor blood glucose control may indicate a need for further evaluation or more frequent monitoring to determine if the disease process interferes with safe driving. Blood glucose levels that remain within the 100 milligrams per deciliter (mg/dL) to 400 mg/dL range are generally considered safe for commercial driving. Oral Hypoglycemics Hypoglycemic drugs taken orally are frequently prescribed for persons with diabetes mellitus to help stimulate natural body production of insulin. Page 180 of 260 Waiting Period No recommended time frame You should not certify the driver until the treatment has been shown to be adequate/effective, safe, and stable. Recommend not to certify if: As a medical examiner, you believe that the nature and severity of the medical condition and/or the treatment of the driver endangers the safety and health of the driver and the public. You may require the driver to have more frequent physical examinations, if indicated, to adequately monitor driver medical fitness for duty. Other Diseases the fundamental question when deciding if a commercial driver should be certified is whether the driver has a condition that so increases the risk of sudden death or incapacitation that the condition creates a danger to the safety and health of the driver, as well as to the public sharing the road. You are expected to assess the nature and severity of the medical condition and determine certification outcomes on a case-by-case basis and with knowledge of the demands of commercial driving. You should not certify the driver until the etiology is confirmed, and treatment has been shown to be adequate/effective, safe, and stable. As the medical examiner, your fundamental obligation during the medical assessment is to establish whether a driver has any disease or disorder that increases the risk for sudden death or incapacitation, thus endangering public safety. Additional questions should be asked, to supplement information requested on the form, to adequately assess medical fitness for duty of the driver. Advisory Criteria/Guidance Hernia the Medical Examination Report form physical examination section includes checking for hernia for both the abdomen and viscera body system and the genitourinary system. Waiting Period No recommended time frame You should not certify the driver until the etiology is confirmed, and treatment has been shown to be adequate/effective, safe, and stable. Decision Maximum certification - 2 years Recommend to certify if: As the medical examiner, you believe that the nature and severity of the medical condition of the driver does not endanger the safety and health of the driver and the public. Monitoring/Testing You may, on a case-by-case basis, obtain additional tests and/or consultation to adequately assess driver medical fitness for duty.
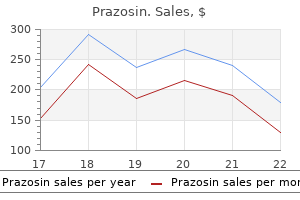
2.5 mg prazosin fast delivery. DD#2: Does the size of an LDL particle matter?.
In addition cholesterol chart in indian food cheap 5mg prazosin overnight delivery, the wedged mirror leads to an undesired angular dispersion of the beam cholesterol levels risk ratio buy prazosin 2.5mg mastercard. However food high in cholesterol shrimp purchase prazosin 2.5mg mastercard, under p-polarized incidence the index contrast and therefore the Fresnel reflectivity of a layer pair is reduced cholesterol ratio of 3.2 order prazosin 2.5 mg online, and more layer pairs are necessary to achieve high reflectivity. This increases the penetration depth into the mirror, which has the advantage that these mirrors can produce more dispersion per reflection, but this means that scattering and other losses, and also fabrication tolerances, become even more severe. In addition, the spatial chirp of the reflected beam has to be removed by back reflection or an additional reflection from another Brewster-angle mirror. Some tuning of the oscillation peaks can be obtained by the angle of incident [22]. Also, this design has its drawbacks and limitations because it requires an extremely high precision in fabrication and restricts the range of angles of incidence. After this overview it becomes clear that there is no perfect solution to the challenge of ultrabroadband dispersion compensation. At this point ultrabroadband chirped mirrors are the only way to compress pulses in the one- to twooptical-cycle regime [25]. A double-chirped dispersive semiconductor mirror has also been demonstrated [138], and a saturable absorber could be integrated into such a device. The first is a transverse index gradient, resulting from the higher intensities on the beam axis compared to the intensities in the wings of the transverse beam profile. This leads to a so-called Kerr lens with an intensity-dependent focusing effect (for positive, n2) which can be exploited for a passive mode-locking mechanism as discussed in Subsection 7. Note that the peak intensity of a Gaussian beam is I = P/(w2/2), and the on-axis phase change (and not an averaged phase change) is relevant for freely propagating beams. For guided beams, an averaged phase change has to be used that is two times smaller. The simple picture of the Kerr nonlinearity as presented above is often sufficient for describing nonlinear effects in mode-locked laser cavities. Besides, the nonlinear response of transparent media also has a noninstantaneous part, which results in the Raman effect. This can lead to the Raman self-frequency shift [139], as can be relevant in mode-locked fiber lasers, for example, but only rarely in bulk lasers. A special case is that the intensity has a sech2 temporal profile P(t) = Pp sech 2 (t / S) = Pp cosh (t / S) 2 (7. Such a pulse propagates in the medium with constant temporal and spectral shape, and only acquires an overall nonlinear phase shift. Higher-order solitons, where the peak power is higher by a factor that is the square of an integer number, do not preserve their temporal and spectral shape but evolve in such a way that the original shape is restored after a certain propagation distance, the so-called soliton period in the case of a second-order soliton. In particular, stable soliton-like pulses can be formed in a laser cavity although dispersion and Kerr nonlinearity occur in discrete amounts, and the pulse energy varies due to amplification in the gain medium and loss in other elements. Note that soliton effects can fix the pulse duration at a certain value even if other cavity elements (most frequently the laser gain with its limited bandwidth) tend to reduce the pulse bandwidth. In this regime of operation, usually a single short pulse propagates in the laser cavity and generates an output pulse each time when it hits the output coupler mirror. In the frequency domain, mode locking means operation of the laser on a number of axial cavity modes, where all these modes oscillate in phase (or at least with nearly equal phases). The term mode locking resulted from the observation that a fixed phase relationship between the modes has to be maintained in some way to produce short pulses. The achievable pulse duration is then inversely proportional to the locked bandwidth, i. It is obvious in the frequency domain description that mode locking cannot be achieved if a significant amount of the laser power is contained in higherorder transverse modes of the cavity, because these usually have different resonance frequencies, so that the periodic recurrence of constructive addition of all mode amplitudes is not possible. In some cases, a mode-locked laser is operated with several equally spaced pulses circulating in the cavity. This mode of operation, called harmonic mode locking [18], can be used for the generation of pulse trains with higher repetition rates even if the cavity can not be made very short (as. The main difficulty is that the timing between the pulses has to be maintained in some way, either by some kind of interaction between the pulses or with the aid of an externally applied timing information.

References
- Koplay M, Kantarci M, Guven F, et al: Diagnostic accuracy of multidetector computed tomography with multiplanar reformatted imaging and virtual cystoscopy in the assessment of bladder tumors after transurethral resection, J Comput Assist Tomogr 34(1):121n126, 2010.
- Areia M, Carvalho R, Cadime AT, et al. Screening for gastric cancer and surveillance of premalignant lesions: a systematic review of cost-effectiveness studies. Helicobacter 2013;18(5):325-337.
- Razvi SS, Bone I. Neurological consultations in the medical intensive care unit. J Neurol Neurosurg Psychiatry. 2003;74(suppl 3):iii-16-iii-23.
- Xiong ZG, Chu XP, Simon RP. Acid sensing ion channels -novel therapeutic targets for ischemic brain injury. Front Biosci 2007;12:1376-86.
- Mizel MS, Yodlowski ML. Disorders of the lesser metatarsophalangeal joints. J Am Acad Orthop Surg. 1995;3(3):166-173.
- Niwa K, Perloff Jk, Bhuta SM, et al. Structural abnormalities of the great arterial walls in congenital heart disease: light and electron microscopic analyses. Circulation. 2001;103:393-400.














